The number should be read as a service-capacity signal, not as a diagnosis of 1 million individual new illnesses. NHS England's mental-health statistics distinguish between referrals, contacts and people in contact with services, and those categories do different work. Referrals show the pressure arriving at the system; treatment data and waiting-time measures show whether the system converts that pressure into help.
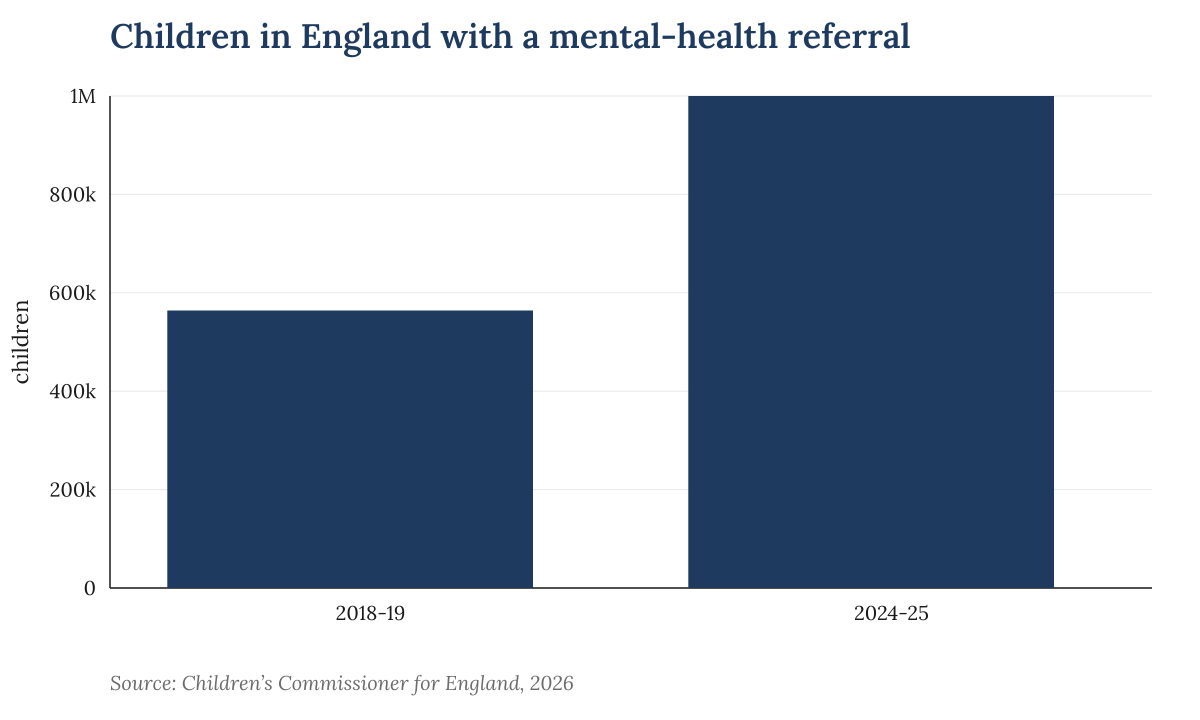 Children in England with a mental-health referral. Source: Children's Commissioner for England, 2026.
Children in England with a mental-health referral. Source: Children's Commissioner for England, 2026.
That distinction is the policy point. A referral is the moment a child is placed into the queue. It does not mean the child has been seen quickly, received a course of treatment, or had the need resolved. If referrals rise faster than clinical workforce, appointment capacity and community support, the visible statistic can improve in one sense while the lived experience worsens: more children are identified, but more wait.
The children's commissioner's analysis gives the trend its political force because it tracks a defined group across several years rather than relying on isolated warnings from individual trusts. The Guardian said the 2024-25 total was nearly twice the 2018-19 level. That makes the issue harder to treat as a short post-pandemic bulge, even though pandemic-era disruption remains part of the context for child and adolescent mental health.
NHS England's monthly mental-health publications are the source that should govern the operational debate. They allow ministers, commissioners and local services to be tested on what happens after referral: how many children are in contact with services, how long they wait, and whether demand is concentrated in particular age groups or regions. A national total is a warning light; the management question sits beneath it.